Medical Billing and Coding Careers Increase Your Career Potential Become a well-rounded resource in the healthcare community by maximizing your career potential as a medical Billing and Coding specialist. Be prepared to be a vital part of any hospital, clinic and healthcare facility nationwide - medical Billing and Coding careers open the door to many career paths!
Medical Billing and Coding Careers Increase Your Career Potential Become a well-rounded resource in the healthcare community by maximizing your career potential as a medical Billing and Coding specialist. Be prepared to be a vital part of any hospital, clinic and healthcare facility nationwide - medical Billing and Coding careers open the door to many career paths!A medical Coding and Billing specialist is responsible for accurately recording and processing data about patients, such as treatment records, insurance information, bills and payments. As a biller and coder, you will code a patient's treatment and diagnosis, and request payments from the insurance company or directly from the individual - you'll play an essential part in the billing cycle from beginning to end!
Yolanda Coar was 40 when she died of COVID-19 in August 2020 in Augusta, Georgia. She was also a nurse manager, and one of nearly 3,000 frontline workers who have died in the U.S. fighting this virus, according to an exclusive investigation by The Guardian and KHN.
Read more of the health workers’ stories behind the statistics — their personalities, passions and quirks. “Lost on the Frontline” examines: Did they have to die?
ERIE, Colo. — Whenever Larry Kelderman looks up from the car he’s fixing and peers across the street, he’s looking across a border. His town of 28,000 straddles two counties, separated by County Line Road.
Kelderman’s auto repair business is in Boulder County, whose officials are sticklers for public health and have topped the county website with instructions on how to report COVID violations. Kelderman lives in Weld County, where officials refuse to enforce public health rules.
Weld County’s test positivity rate is twice that of its neighbor, but Kelderman is pretty clear which side he backs.
“Which is worse, the person gets the virus and survives and they still have a business, or they don’t get the virus and they lose their livelihood?” he said.
Boulder boasts one of the most highly educated populations in the nation; Weld boasts about its sugar beets, cattle and thousands of oil and gas wells. Summer in Boulder County means concerts featuring former members of the Grateful Dead; in Weld County, it’s rodeo time. Boulder voted for Biden, Weld for Trump. Per capita income in Boulder is nearly 50% higher than in Weld.
Even their COVID outbreaks are different: In Boulder County, the virus swirls around the University of Colorado. In Weld County, some of the worst outbreaks have swept through meatpacking plants.
The town of Erie, Colorado, straddles two counties with opposite views on how to approach COVID-19. (Rae Ellen Bichell/KHN)
It’s not the first time County Line Road has been a fault line.
“I’ve been in politics seven years and there’s always been a conflict between the two counties,” said Jennifer Carroll, mayor of Erie, once a coal mining town and now billed as a good place to raise a family, about 30 minutes north of Denver.
Shortly before the coronavirus hit Colorado, Erie’s board of trustees extended a moratorium on new oil and gas operations in the town. Weld County was not pleased.
“They got really angry at us for doing that, because oil and gas is their thing,” Carroll said.
Most of the town’s businesses are on the Weld side. To avoid public health whiplash, Carroll and other town leaders have asked residents to comply with the more restrictive stance of the Boulder side.
The feud got ugly in a dispute over hospital beds. At one point, the state said Weld County had only three intensive care beds, while Weld County claimed it had 43.
“It made my job harder, because people were doubting what I was saying,” said Carroll. “Nobody trusted anyone because they were hearing conflicting information.”
Weld’s number, it turned out, included not just the beds in its two hospitals, but also those in 10 other hospitals across the county line, including in the city of Longmont.
Longmont sits primarily in Boulder County but spills into Weld, where its suburbs taper into fields pockmarked with prairie dog holes. Its residents say they can tell snow is coming when the winds deliver a pungent smell of livestock from next door. Longmont Mayor Brian Bagley worried that Weld’s behavior would deliver more than a stench: It might also deliver patients requiring precious resources.
“They were basically encouraging their citizens to violate the emergency health orders … with this cowboy-esque, you know, ‘Yippee-ki-yay, freedom, Constitution forever, damn the consequences,’” said Bagley. “Their statement is, ‘Our hospitals are full, but don’t worry, we’re just going to use yours.’”
So, “for 48 hours, I trolled Weld County,” he said. Bagley asked the city council to consider an ordinance that could have restricted Weld County residents’ ability to receive care at Longmont hospitals. Bagley, who retracted his proposal the next day, said he knew it was never going to come to fruition — after all, it was probably illegal — but he wanted to prove a point.
“They’re going to be irresponsible? Fine. Let me propose a question,” he said. “If there is only one ICU bed left and there are two grandparents there — one from Weld, one from Boulder — and they both need that bed, who should get it?”
Weld County commissioners volleyed back, calling Bagley a “simple mayor.” They wrote that the answer to the pandemic was “not to continually punish working-class families or the individuals who bag your groceries, wait on you in restaurants, deliver food to your home while you watch Netflix and chill.”
“I know we’re all trying to get along, but people are starting to do stupid and mean things and so I’ll be stupid and mean back,” Bagley said during a Dec. 8 council meeting.
In another Longmont City Council meeting, Bagley (who suspects the commissioners don’t know what “Netflix and chill” typically means) often referred to Weld simply as “our neighbors to the East,” declining to name his foe. The council shrugged off his statement about withholding medical treatment but demanded that Weld County step up to fight the pandemic.
“We would not deny medical care to anybody. It’s illegal and it’s immoral,” said council member Polly Christensen. “But it is wrong for people to expect us to bear the burden of what they’ve been irresponsible enough to let loose.”
“They’re the reason why I can’t be in the classroom in front of my kids,” said council member and teacher Susie Hidalgo-Fahring, whose school district straddles the counties. “I’m done with that. Everybody needs to be a good neighbor.”
County Line Road is not just a street cutting through Erie, Colorado. It represents a fault line between local governments with very different views on the pandemic. (Rae Ellen Bichell/KHN)
Josh Kelderman works with his father, Larry, at the family’s auto repair business, Integrity Products, on the Boulder County side of Erie, Colorado. Weld County is just across the street. (Rae Ellen Bichell/KHN)
The council decided Dec. 15 to send a letter to Weld County’s commissioners encouraging them to enforce state restrictions and to make a public statement about the benefits of wearing masks and practicing physical distancing. They’ve also backed a law allowing Democratic Gov. Jared Polisto withhold relief money from counties that don’t comply with restrictions.
Weld County Commissioner Scott James said his county doesn’t have the authority to enforce public health orders any more than a citizen has the authority to give a speeding ticket.
“If you want me as an elected official to assume authority that I don’t have and arbitrarily exert it over you, I dare you to look that up in the dictionary,” said James, who is a rancher turned country radio host. “It’s called tyranny.”
James doesn’t deny that COVID-19 is ravaging his community. “We’re on fire, and we need to put that fire out,” he said. But he believes that individuals will make the right decisions to protect others, and demands the right of his constituents to use the hospital nearest them.
“To look at Weld County like it has walls around it is shortsighted and not the way our health care system is designed to work,” James said. “To use a crudity, because I am, after all, just a ranch kid turned radio guy, there’s no ‘non-peeing’ section in the pool. Everybody’s gonna get a little on ’em. And that’s what’s going on right now with COVID.”
The dispute is not just liberal and conservative politics clashing. Bagley, the Longmont mayor, grew up in Weld County and “was a Republican up until Trump,” he said. But it is an example of how the virus is tapping into long-standing Western strife.
“There’s decades of reasons for resentment at people from a distance — usually from a metropolis and from a state or federal governmental office — telling rural people what to do,” said Patty Limerick, faculty director at the Center of the American West at the University of Colorado-Boulder, and previously state historian.
In the ’90s, she toured several states performing a mock divorce trial between the rural and urban West. She played Urbana Asphalt West, married to Sandy Greenhills West. Their child, Suburbia, was indulged and clueless and had a habit of drinking everyone else’s water. A rural health care shortage was one of many fuels of their marital strife.
Limerick and her colleagues are reviving the play now and adding COVID references. This time around, she said, it’ll be a last-ditch marriage counseling session for high school classes and communities to adopt and perform. It likely won’t have a scripted ending; she’s leaving that up to each community.
Nine months into the pandemic that has killed more than 320,000 people in the U.S., Kim Larson is still trying to convince others in her northern Montana county that COVID-19 is dangerous.
As Hill County Health Department director and county health officer, Larson continues to hear people say the coronavirus is just like a bad case of the flu. Around the time Montana’s governor mandated face coverings in July, her staffers saw notices taped in several businesses’ windows spurning the state’s right to issue such emergency orders.
For a while, the county with a population of 16,000 along the Canadian border didn’t see much evidence of the pandemic. It had only one known COVID case until July. But that changed as the nation moved into its third surge of the virus this fall. By mid-December, Hill County had recorded more than 1,500 cases — the vast majority since Oct. 1 — and 33 people there had died.
When Larson hears people say pandemic safety rules should end, she talks about how contagious the COVID virus is, how some people experience lasting effects and how hospitals are so full that care for any ailment could face delays.
“In public health, we’ve seen the battle before, but you typically have the time to build your evidence, research showing that this really does save lives,” Larson said. “In the middle of a pandemic, you have no time.”
Public health laws typically come long after social norms shift, affirming a widespread acceptance that a change in habits is worth the public good and that it’s time for stragglers to fall in line. But even when decades of evidence show a rule can save lives — such as wearing seat belts or not smoking indoors — the debate continues in some places with the familiar argument that public restraints violate personal freedoms. This fast-moving pandemic, however, doesn’t afford society the luxury of time. State mandates have put local officials in charge of changing behavior while general understanding catches up.
Earlier this month, U.S. Surgeon General Jerome Adams stood next to Montana’s governor in Helena and said he hopes people wear masks because it’s the right thing to do — especially as COVID hospitalizations rise.
“You don’t want to be the reason that a woman in labor can’t get a hospital bed,” Adams said, adding a vaccine is on the way. “It’s just for a little bit longer.”
He spoke days after state lawmakers clashed over masks as a majority of Republican lawmakers arrived for a committee meeting barefaced and at least one touted false information on the dangers of masks. As of Dec. 15, the Republican majority hadn’t required masks for the upcoming legislative session, set to begin Jan. 4.
And now a group opposed to masks from Gallatin and Flathead counties has filed a lawsuit asking a Montana judge to block the state’s pandemic-related safety rules.
Public health laws typically spark political battles. Changing people’s habits is hard, said Lindsay Wiley, director of the health law and policy program at American University in Washington, D.C. Despite the misconception that there was universal buy-in for masks during the 1918 pandemic, Wiley said, some protesters intentionally built rap sheets of arrests for going maskless in the name of liberty.
She said health officials realize any health restrictions amid a pandemic require the public’s trust and cooperation for success.
“We don’t have enough police to walk around and force everyone to wear a mask,” she said. “And I’m not sure we want them to do it.”
Local officials have the best chance to win over that support, Wiley said. And seeing elected leaders such as President Donald Trump rebuff his own federal health guidelines makes that harder. Meanwhile, public shaming like calling unmasked people selfish or stupid can backfire, Wiley said, because if they were to give in to mask-wearing, they would essentially be accepting those labels.
In the history of public health laws, even rules that have had time to build widely accepted evidence weren’t guaranteed support.
It’s illegal in Montana to go without a seat belt in a moving car. But, as in 13 other states, authorities aren’t allowed to pull people over for being unbuckled. Every few years, a Montana lawmaker, backed by a collection of public health and law enforcement organizations, proposes a law to allow seat belt traffic stops, arguing it would save lives. In 2019, that request didn’t even make it out of committee, squelched by the arguments of personal choice and not giving too much power to the government.
Main opposition points against public health laws — whether it’s masks, seat belts, motorcycle helmets or smoking — can sound alike.
When Missoula County became the first place in Montana to ban indoor smoking in public spaces in 1999, opponents said the change would destroy businesses, be impossible to enforce and violate people’s freedom of choice.
“They are the same arguments in a lot of ways,” said Ellen Leahy, director of the Missoula City-County Health Department. “Public health was right at that intersection between what’s good for the whole community and the rights and responsibilities of the individual.”
Montana adopted an indoor smoking ban in 2005, but many bars and taverns were given until 2009 to fall in line. And, in some places, debate and court battles continued for a decade more on how the ban could be enforced.
Amid the COVID pandemic, Missoula County was again ahead of much of the state when it passed its own mask ordinance. The county has two hospitals and a university that swells its population with students and commuters.
“If you have to see it to believe it, you’re going to see the impact of a pandemic first in a city, most likely,” Leahy said.
Compliance hasn’t been perfect and she said the need for strict enforcement has been limited. As of early December, out of the more than 1,500 complaints the Missoula health department followed up on since July, it sent closure notices to four businesses that flouted the rules.
In Hill County, when the health department gets complaints that a business is violating pandemic mandates, two part-time health sanitarians, who perform health inspections of businesses, talk with the owners about why the rules exist and how to live by them. Often it works. Other times the complaints keep coming.
County attorney Karen Alley said the local health officials have reached out to her office with complaints of noncompliance on COVID safety measures, but she has not seen enough evidence to bring a civil case against a business. Unlike other health laws, she said, mask rules have no case studies yet to offer a framework for enforcing them through the Montana courts. (A handful of cases against businesses skirting COVID rules were still playing out as of mid-December.)
“Somebody has to be the test case, but you never want to be the test case,” said Alley, who is part of a team of three. “It’s a lot of resources, a lot of time.”
Larson, with the Hill County Health Department, said her focus is still on winning over the community. And she’s excited about some progress. The town’s annual live Nativity scene, which typically draws crowds with hot cocoa, turned into a drive-by event this year.
She doesn’t expect everyone to follow the rules — that’s never the case in public health. But Larson hopes enough people will to slow down the virus. That could be happening. By mid-December, the county’s tally of daily active cases was declining for the first time since its spike began in October.
“You just try to figure out the best way for your community and to get their input,” Larson said. “Because we need the community’s help to stop it.”
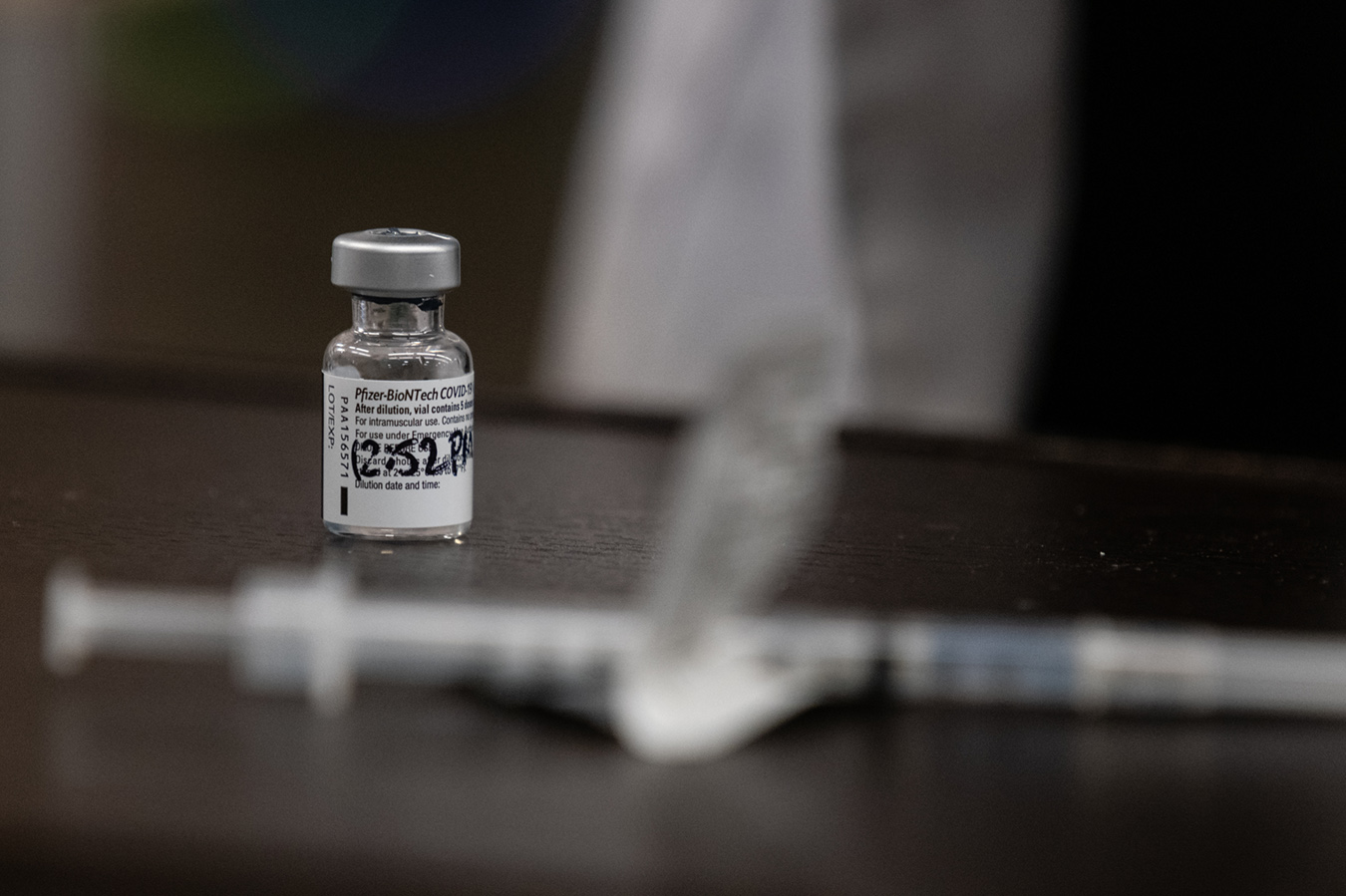
WASHINGTON — Even before there was a vaccine, some seasoned doctors and public health experts warned, Cassandra-like, that its distribution would be “a logistical nightmare.”
After Week 1 of the rollout, “nightmare” sounds like an apt description.
Dozens of states say they didn’t receive nearly the number of promised doses. Pfizer says millions of doses sat in its storerooms, because no one from President Donald Trump’s Operation Warp Speed task force told them where to ship them. A number of states have few sites that can handle the ultra-cold storage required for the Pfizer product, so, for example, front-line workers in Georgia have had to travel 40 minutes to get a shot. At some hospitals, residents treating COVID patients protested that they had not received the vaccine while administrators did, even though they work from home and don’t treat patients.
The potential for more chaos is high. Dr. Vivek Murthy, named as the next surgeon general under President-elect Joe Biden, said this week that the Trump administration’s prediction — that the general population would get the vaccine in April — was realistic only if everything went smoothly. He instead predicted wide distribution by summer or fall.
The Trump administration had expressed confidence that the rollout would be smooth, because it was being overseen by a four-star general, Gustave Perna, an expert in logistics. But it turns out that getting fuel, tanks and tents into war-torn mountainous Afghanistan is in many ways simpler than passing out a vaccine in our privatized, profit-focused and highly fragmented medical system. Gen. Perna apologized this week, saying he wanted to “take personal responsibility.” It’s really mostly not his fault.
Throughout the COVID pandemic, the U.S. health care system has shown that it is not built for a coordinated pandemic response (among many other things). States took wildly different COVID prevention measures; individual hospitals varied in their ability to face this kind of national disaster; and there were huge regional disparities in test availability — with a slow ramp-up in availability due, at least in some part, because no payment or billing mechanism was established.
Why should vaccine distribution be any different?
In World War II, toymakers were conscripted to make needed military hardware airplane parts, and commercial shipyards to make military transport vessels. The Trump administration has been averse to invoking the Defense Production Act, which could help speed and coordinate the process of vaccine manufacture and distribution. On Tuesday, it indicated it might do so, but only to help Pfizer obtain raw materials that are in short supply, so that the drugmaker could produce — and sell — more vaccines in the United States.
Instead of a central health-directed strategy, we have multiple companies competing to capture their financial piece of the pandemic health care pie, each with its patent-protected product as well as its own supply chain and shipping methods.
Add to this bedlam the current decision-tree governing distribution: The Centers for Disease Control and Prevention has made official recommendations about who should get the vaccine first — but throughout the pandemic, many states have felt free to ignore the agency’s suggestions.
Instead, Operation Warp Speed allocated initial doses to the states, depending on population. From there, an inscrutable mix of state officials, public health agencies and lobbyists seem to be determining where the vaccine should go. In some states, counties requested an allotment from the state, and then they tried to accommodate requests from hospitals, which made their individual algorithms for how to dole out the precious cargo. Once it became clear there wasn’t enough vaccine to go around, each entity made its own adjustments.
Some doses are being shipped by FedEx or UPS. But Pfizer — which did not fully participate in Operation Warp Speed — is shipping much of the vaccine itself. In nursing homes, some vaccines will be delivered and administered by employees of CVS and Walgreens, though issues of staffing and consent remain there.
The Moderna vaccine, rolling out this week, will be packaged by the “pharmaceutical services provider” Catalent in Bloomington, Indiana, and then sent to McKesson, a large pharmaceutical logistics and distribution outfit. It has offices in places like Memphis, Tennessee, and Louisville, which are near air hubs for FedEx and UPS, which will ship them out.
Is your head spinning yet?
Looking forward, basic questions remain for 2021: How will essential workers at some risk (transit workers, teachers, grocery store employees) know when it’s their turn? (And it will matter which city you work in.) What about people with chronic illness — and then everyone else? And who administers the vaccine — doctors or the local drugstore?
In Belgium, where many hospitals and doctors are private but work within a significant central organization, residents will get an invitation letter “when it’s their turn.” In Britain, the National Joint Committee on Vaccination has settled on a priority list for vaccinations — those over 80, those who live or work in nursing homes, and health care workers at high risk. The National Health Service will let everyone else “know when it’s your turn to get the vaccine ” from the government-run health system.
In the United States, I dread a mad scramble — as in, “Did you hear the CVS on P Street got a shipment?” But this time, it’s not toilet paper.
Combine this vision of disorder with the nation’s high death toll, and it’s not surprising that there is intense jockeying and lobbying — by schools, unions, even people with different types of preexisting diseases — over who should get the vaccine first, second and third. It’s hard to “wait your turn” in a country where there are 200,000 new cases and as many as 2,000 new daily COVID deaths — a tragic per capita order of magnitude higher than in many other developed countries.
So kudos and thanks to the science and the scientists who made the vaccine in record time. I’ll eagerly hold out my arm — so I can see the family and friends and colleagues I’ve missed all these months. If only I can figure out when I’m eligible, and where to go to get it.
El reciente lanzamiento de dos vacunas para COVID-19 es una luz de esperanza en medio de la pandemia.
Ahora hay un camino que puede llevarnos a tiempos más felices, incluso mientras observamos y sufrimos la horrible avalancha de nuevas infecciones, hospitalizaciones y muertes que marcan el final de este año lamentable.
Los trabajadores de salud y los residentes de hogares de adultos mayores ya han comenzado a recibir vacunas en la primera fase de la distribución. Y más deberían estar disponibles para el público en general en los primeros meses del próximo año.
Las dos vacunas, una desarrollada por Pfizer y BioNTech, la otra por Moderna, utilizan el mismo enfoque genético novedoso. Su desarrollo en menos de un año, rompiendo todos los récords, es una maravilla de la ciencia. También es motivo de preocupación para millones de estadounidenses que sienten incertidumbre ante una tecnología desconocida.
Los datos de los ensayos clínicos de Las vacunas de Pfizer y Moderna muestran que cuando se reciben las dos dosis necesarias, con un intervalo de tres semanas a un mes, tienen una eficacia de aproximadamente el 95%, al menos para prevenir la forma grave de COVID.
Sin embargo, “una vacuna que permanece en el frasco tiene un 0% de efectividad sin importar lo que muestren los datos”, dijo el doctor Walter Orenstein, profesor de enfermedades infecciosas en la Escuela de Medicina de la Universidad de Emory en Atlanta y director asociado del Centro de Vacunas Emory.
De ahí la importancia de persuadir a millones de personas, de todas las razas, culturas, religiones, simpatías políticas y edades, para que se vacunen cuando llegue el momento. Una encuesta publicada este mes mostró que el 45% de los encuestados están adoptando un enfoque de “esperar y ver qué pasa” con la vacunación.
Debido a que las vacunas se desarrollaron bajo la presión de una pandemia mortal, la clave fue la velocidad. Por lo que, aunque el número de personas en los ensayos es tan grande o mayor que en pruebas anteriores, algunas preguntas clave no se responderán hasta que se vacunen millones más.
Por ejemplo, no se sabe si podrían surgir efectos secundarios irreversibles o quién corre mayor riesgo de sufrirlos. Y tampoco si habrá que vacunarse todos los años, cada tres años o nunca más.
Estas incógnitas se suman a los desafíos que enfrentan el gobierno federal, autoridades de salud locales, profesionales médicos y entidades privadas mientras buscan persuadir a la mayor cantidad de personas posible para que se vacunen.
Hay escepticismo en muchos sectores, incluso entre los afroamericanos, que desconfían desde hace mucho tiempo del mundo médico; los ruidosos “anti-vacunas”; y gente con dudas perfectamente comprensibles. Sin mencionar las comunidades con barreras idiomáticas e inmigrantes indocumentados, más de 2 millones solo en California, que pueden temer ir al centro de vacunación.
A continuación, respuestas a algunas preguntas sobre las nuevas vacunas:
¿Cómo puedo saber si son seguras?
No hay una garantía absoluta. Pero al autorizar las vacunas de Pfizer y Moderna, la Administración de Drogas y Alimentos (FDA) determinó que sus beneficios superaban a sus riesgos.
Los efectos secundarios observados en los participantes delos ensayos fueron similares a los de otras vacunas: dolor en el lugar de la inyección, fatiga, dolor de cabeza, dolor muscular y escalofríos. “Esos son efectos secundarios menores y el beneficio es no morir a causa de esta enfermedad”, dijo el doctor George Rutherford, profesor de Epidemiología en la Universidad de California-San Francisco.
Es posible que aparezcan otros efectos adversos inesperados en el futuro. “Las posibilidades son bajas, pero no nulas”, dijo Orenstein. Por ejemplo, todavía no hay datos suficientes para saber si las vacunas representan un riesgo elevado para las mujeres embarazadas o lactantes, o para las personas inmunodeprimidas, como las que viven con VIH.
Y sabemos muy poco sobre los efectos en los niños, que no formaron parte de los ensayos iniciales y para quienes las vacunas no están autorizadas.
¿Por qué debería vacunarse una familia?
En primer lugar, porque se protegerán de la posibilidad de una enfermedad grave o incluso de la muerte. Además, al vacunarse estarán haciendo su parte para lograr una tasa de vacunación lo suficientemente alta como para poner fin a la pandemia. Nadie sabe exactamente qué porcentaje de la población necesita vacunarse para que eso suceda, pero expertos en enfermedades infecciosas sitúan la cifra entre el 60% y el 70%, quizás incluso un poco más. Hay que pensar en vacunarse como en un deber cívico.
Entonces, ¿cuando vacunarse?
Depende del estado de salud de la persona, edad y trabajo. En la primera fase, que ya está en marcha, se está vacunando a trabajadores de salud y a adultos mayores en hogares. Las 40 millones de dosis de Moderna y Pfizer que se espera estén disponibles para fin de año deberían inmunizar a la mayoría de ellos.
Es posible que haya suficientes vacunas disponibles para el resto de la población a fines de la primavera, pero es más probable el verano o incluso el otoño. Ya se han desarrollado algunos cuellos de botella en la distribución.
En el lado positivo, otras dos vacunas, una de Johnson & Johnson, la otra de AstraZeneca y la Universidad de Oxford, podrían obtener la autorización de la FDA a principios del próximo año, aumentando significativamente el suministro.
Una vez que la persona se vacuna, ¿puede dejar de usar una máscara y el distanciamiento físico?
No. Especialmente al principio, antes de que muchas personas hayan sido vacunadas. Una de las razones es la autoprotección. Las vacunas de Moderna y Pfizer tienen una efectividad del 95%, pero eso significa que la persona aún tiene un 5% de posibilidades de enfermarse si está expuesta a alguien con COVID.
Si la persona ya tuvo COVID-19, ¿aún necesita vacunarse?
Todavía no se sabe con certeza cuánto tiempo dura la inmunidad luego de la infección, y si hay posibilidad de reinfección. Expertos en salud pública dicen que es buena idea vacunarse cuando llegue el turno, especialmente si han pasado muchos meses desde que la persona dio positivo.
Se ha hablado de que las personas que ya han tenido COVID estén últimos en la fila para recibir la vacuna, para garantizar un suministro adecuado para aquellos que podrían estar en mayor riesgo.
¿Cuánto tiempo pasará antes de que se vuelva a la normalidad?
“Si todo va bien, el próximo Día de Acción de Gracias podría ser casi normal y podríamos estar acercándonos a eso para el verano”, dice el doctor William Schaffner, profesor de enfermedades infecciosas en la Escuela de Medicina de la Universidad de Vanderbilt en Nashville, Tennessee. “Pero tendría que haber una aceptación sustancial de la vacuna y datos que muestren que el virus se mueve en una dirección descendente”.
In late summer, as researchers accelerated the first clinical trials of COVID-19 vaccines for humans, a group of scientists in Colorado worked to inoculate a far more fragile species.
About 120 black-footed ferrets, among the most endangered mammals in North America, were injected with an experimental COVID vaccine aimed at protecting the small, weasel-like creatures rescued from the brink of extinction four decades ago.
The effort came months before U.S. Department of Agriculture officials began accepting applications from veterinary drugmakers for a commercial vaccine for minks, a close cousin of the ferrets. Farmed minks, raised for their valuable fur, have died by the tens of thousands in the U.S. and been culled by the millions in Europe after catching the COVID virus from infected humans.
Vaccinating such vulnerable species against the disease is important not only for the animals’ sake, experts say, but potentially for the protection of people. Some of the most pernicious human diseases have originated in animals, including the new coronavirus, which is believed to have spread from bats to an intermediary species before jumping to humans and sparking the pandemic.
The worry when it comes to animals like farmed minks, which are kept in crowded pens, is that the virus, contracted from humans, can mutate as it spreads rapidly in the susceptible animals, posing a new threat if it spills back to people. Danish health officials in November reported detecting more than 200 COVID cases in humans that had variants associated with farmed minks, including a dozen with a mutation scientists feared could undermine the effectiveness of vaccines. However, officials now say that variant appears to be extinct.
In the U.S., scientists have not found similar COVID mutations in the domestic farmed mink populations, though they recently noted with concern the discovery of the first case of the virus in a wild mink in Utah.
“For highly contagious respiratory viruses, it’s really important to be mindful of the animal reservoir,” said Dr. Corey Casper, a vaccinologist and chief executive of the Infectious Disease Research Institute in Seattle. “If the virus returns to the animal host and mutates, or changes, in such a way that it could be reintroduced to humans, then the humans would no longer have that immunity. That makes me very concerned.”
For the newly vaccinated ferrets, the main risk is to the animals themselves. They’re part of a captive population at the National Black-footed Ferret Conservation Center outside Fort Collins, Colorado, where there have been no cases of COVID-19 to date. But the slender, furry creatures — known for their distinctive black eye mask, legs and feet — are feared to be highly vulnerable to the ravages of the disease, said Tonie Rocke, a research scientist at the National Wildlife Health Center who is testing the ferret vaccine. They’re all genetically similar, having come from a narrow breeding pool, which weakens their immune systems. And they likely share many of the features that have made the disease so deadly to minks.
“We don’t have direct evidence that black-footed ferrets are susceptible to COVID-19, but given their close relationship to minks, we wouldn’t want to find out,” Rocke said.
Rocke began working on the experimental vaccine in the spring, as she and Pete Gober, black-footed ferret recovery coordinator for the U.S. Fish and Wildlife Service, watched reports about the new coronavirus with growing alarm. An exotic disease is “the biggest nemesis for ferret recovery,” said Gober, who has worked with black-footed ferrets for 30 years. “It can knock you right back down to zero.”
Pete Gober, coordinator for the U.S. Fish and Wildlife Service’s black-footed ferret recovery program, pictured in 2016. (Ryan Moehring / USFWS via flickr)
The ferrets are a native species that once roamed vast areas of the American West. Their ranks declined precipitously over many decades as populations of prairie dogs, the ferrets’ primary source of food and shelter, were decimated by farming, grazing and other human activity.
In 1979, black-footed ferrets were declared extinct — until a small population was discovered on a ranch in Wyoming. Most of those rare animals were then lost to disease, including sylvatic plague, the animal version of the Black Death that has plagued humans. The species survived only because biologists rescued 18 ferrets to form the basis of a captive breeding program, Gober said.
With the threat of new disease looming, Gober doubled-down on the strict infection prevention precautions at the center, which houses more than half of the 300 black-footed ferrets in captivity. An additional 400 have been reintroduced to the wild. Then he called Rocke, who previously created a vaccine shown to protect ferrets from sylvatic plague. It uses a purified protein from Yersinia pestis, the bacterium that causes the disease.
Would the same technique work against the virus that causes COVID-19? Under the research authority granted by the Fish and Wildlife Service, the scientists were free to try.
“We can do these sorts of things experimentally in animals that we can’t do in humans,” Rocke noted.
Rocke acquired purified protein of a key component of the SARS-CoV-2 virus, the spike protein, from a commercial producer. She mixed the liquid protein with an adjuvant, a substance that enhances immune response, and injected it under the animals’ skin.
The first doses were given in late spring to 18 black-footed ferrets, all male, all about a year old, followed by a booster dose a few weeks later. Within weeks of getting the second shots, tests of the animals’ blood showed antibodies to the virus, a good — and expected — sign.
By early fall, 120 of the 180 ferrets housed at the center were inoculated, with the rest remaining unvaccinated in case something went wrong with the animals, which generally live four to six years in captivity. So far, the vaccine appears safe, but there’s no data yet to show whether it protects the animals from disease. “I can tell you, we have no idea if it will work,” said Rocke, who plans to conduct efficacy tests this winter.
But Rocke’s effort makes sense, said Casper, who has created several vaccines for humans. Rocke’s approach — introducing an inactivated virus in an animal to stimulate an immune response — is the basis for many common vaccines, such as those that prevent polio and influenza.
Vaccines containing inactivated virus to prevent COVID-19 have been tested in certain animals — and in human vaccines, including CoronaVac, created by the Chinese firm Sinovac Life Sciences. But the effort in Colorado may be among the first aimed at preventing COVID-19 in a specific animal population, Rocke said.
Gober said he is optimistic that the ferrets are protected, but it will take a well-designed study to settle the question. Until then, he’ll work to keep the fragile ferrets free of COVID-19. “The price of peace is eternal vigilance, they say. We can’t let our guard down.”
The tougher task is doing the same for people, Gober observed.
“We’re just holding our breath, hoping we can get all the humans vaccinated in the country. That will give us all a sigh of relief.”
Lorraine Rogge and her husband, Michael Rogge, travel the country in a recreational vehicle, a well-earned adventure in retirement. This spring found them parked in Artesia, New Mexico, for several months.
In May, Rogge, 60, began to feel pelvic pain and cramping. But she had had a total hysterectomy in 2006, so the pain seemed unusual, especially because it lasted for days. She looked for a local gynecologist and found one who took her insurance at the Carlsbad Medical Center in Carlsbad, New Mexico, about a 20-mile drive from the RV lot.
The doctor asked if Rogge was sexually active, and she responded yes and that she had been married to Michael for 26 years. Rogge felt she made it clear that she is in a monogamous relationship. The doctor then did a gynecological examination and took a vaginal swab sample for laboratory testing.
The only lab test Rogge remembered discussing with the doctor was to see whether she had a yeast infection. She wasn’t given any medication to treat the pelvic pain and eventually it disappeared after a few days.
Then the bill came.
The Patient: Lorraine Rogge, 60. Her insurance coverage was an Anthem Blue Cross retiree plan through her husband’s former employer, with a deductible of $2,000 and out-of-pocket maximum of $6,750 for in-network providers.
Total Bill: Carlsbad Medical Center billed $12,386.93 to Anthem Blue Cross for a vaginosis, vaginitis and sexually transmitted infections (STI) testing panel. The insurer paid $4,161.58 on a negotiated rate of $7,172.05. That left Rogge responsible for $1,970 of her deductible and $1,040.36 coinsurance. Her total owed for the lab bill was $3,010.47. Rogge also paid $93.85 for the visit to the doctor.
Service Provider:Carlsbad Medical Center in Carlsbad, New Mexico. It is owned by Community Health Systems, a large for-profit chain of hospital systems based in Franklin, Tennessee, outside Nashville. The doctor Rogge saw works for Carlsbad Medical Center and its lab processed her test.
Medical Service: A bundled testing panel that looked for bacterial and yeast infections as well as common STIs, including chlamydia, gonorrhea and trichomoniasis.
What Gives: There were two things Rogge didn’t know as she sought care. First, Carlsbad Medical Center is notorious for its high prices and aggressive billing practices and, second, she wasn’t aware she would be tested for a wide range of sexually transmitted infections.
The latter bothered her a lot since she has been sexually active only with her husband. She doesn’t remember being advised about the STI testing at all. Nor was she questioned about whether she or her husband might have been sexually active with other people, which could have justified broader testing. They have been on the road together for five years.
“I was incensed that they ran these tests, when they just said they were going to run a yeast infection test,” said Rogge. “They ran all these tests that one would run on a very young person who had a lot of boyfriends, not a 60-year-old grandmother that’s been married for 26 years.”
Although a doctor doesn’t need a patient’s authorization to run tests, it’s not good practice to do so without informing the patient, said Dr. Ina Park, an associate professor of family community medicine at the University of California-San Francisco School of Medicine. That is particularly true with tests of a sensitive nature, like STIs. It is doubly true when the tests are going to costs thousands of dollars.
Lorraine and Michael Rogge inside their RV in El Cajon, California.(Heidi de Marco/KHN)
Park, an expert in sexually transmitted infections, also questioned the necessity of the full panel of tests for a patient who had a hysterectomy.
Beyond that, the pricing for these tests was extremely high. “It should not cost $12,000 to get an evaluation for vaginitis,” said Park.
“Quite frankly, the retail prices on [the bill] are ridiculous, they make no sense at all,” said Root. “Those are tests that cost about $10 to run.”
In fall 2019, The New York Times and CNN investigated Carlsbad Medical Center and found the facility had taken thousands of patients to court for unpaid hospital bills. Carlsbad Medical Center also has higher prices than many other facilities — a 2019 Rand Corp. study found that private insurance companies paid Carlsbad Medical Center 505% of what Medicare would pay for the same procedures.
The bundled testing panel run on Rogge’s sample was a Quest Diagnostics SureSwab Vaginosis Panel Plus. It included six types of tests. Quest Diagnostics didn’t provide the cost for the bundled tests, but Kim Gorode, a company spokesperson, said if the tests had been ordered directly through Quest rather than through the hospital, it was likely “the patient responsibility would have been substantially less.”
According to Medicare’s Clinical Laboratory Fee Schedule, Medicare would have reimbursed labs only about $40 for each test run on Rogge’s sample. And Medicaid would reimburse hospitals in New Mexico similarly, according to figures provided by Russell Toal, superintendent of New Mexico’s insurance department.
But hospitals and clinics can — and do — add substantial markups to clinical tests sent out to commercial labs.
Although private health insurance doesn’t typically reimburse hospitals at Medicare or Medicaid rates, Root said, private insurance reimbursement rates are rarely much more than 200% to 300% of Medicare’s rates. Assuming a 300% reimbursement rate, the total private insurance would have reimbursed for the six tests would have been $720.
That $720 is less than what Carlsbad Medical Center charged Rogge for her chlamydia test alone: $1,045. And for several of the tests, the medical center charged multiple quantities — presumably corresponding to how many species were tested for — elevating the cost of the yeast infection test to over $4,000.
Toal, who reviewed Rogge’s bill, called the prices “outrageous.”
Resolution: Rogge contacted Anthem Blue Cross and talked to a customer service representative, who submitted a fraud-and-waste claim and an appeal contending the charges were excessive.
The appeal was denied. Anthem Blue Cross told Rogge that under her plan the insurance company had paid the amount it was responsible for, and that based on her deductible and coinsurance amounts, she was responsible for the remainder.
Anthem Blue Cross said in a statement to KHN all the tests run on Rogge were approved and “paid for in accordance with Anthem’s pre-determined contracted rate with Carlsbad Medical Center.”
By the time Rogge’s appeal was denied, she had researched Carlsbad Medical Center and read the stories of patients being brought to court for medical bills they couldn’t pay. She had also gotten a notice from the hospital that her account would be sent to a collection agency if she didn’t pay the $3,000 balance.
Fearing the possibility of getting sued or ruining her credit, Rogge agreed to a plan to pay the bill over three years. She made three payments of $83.63 each in September, October and November, totaling $250.89.
After a Nov. 18 call and email from KHN, Carlsbad Medical Center called Rogge on Nov. 20 and said the remainder of her account balance would be waived.
Rogge was thrilled. We “aren’t the kind of people who have payment plans hanging over our heads,” she said, adding: “This is a relief.”
“I’m going to go on a bike ride now” to celebrate, she said.
The Takeaway: Particularly when visiting a doctor with whom you don’t have a long-standing trusted relationship, don’t be afraid to ask: How much is this test going to cost? Also ask for what, exactly, are you being tested? Do not be comforted by the facility’s in-network status. With coinsurance and deductibles, you can still be out a lot.
If it’s a blood test that will be sent out to a commercial lab like Quest Diagnostics anyway, ask the physician to just give you a requisition to have the blood drawn at the commercial lab. That way you avoid the markup. This advice is obviously not possible for a vaginal swab gathered in a doctor’s office.
Patients should always fight bills they believe are excessively high and escalate the matter if necessary.
Rogge started with her insurer and the provider, as should most patients with a billing question. But, as she learned: In American medicine, what’s legal and in accordance with an insurance contract can seem logically absurd. Still, if you get no satisfaction from your initial inquiries, be aware of options for taking your complaints further.
Every state and U.S. territory has a department that regulates the insurance industry. In New Mexico, that’s the Office of the Superintendent of Insurance. Consumers can look up their state’s department on the National Association of Insurance Commissioners website.
Toal, the insurance superintendent in New Mexico, said his office doesn’t (and no office in the state does that he’s aware of) have the authority to tell a hospital its prices are too high. But he can look into a bill like Rogge’s if a complaint is filed with his office.
“If the patient wants, they can request an independent review, so the bill would go to an independent organization that could see if it was medically necessary,” Toal said.
That wasn’t needed in this case because Rogge’s bill was waived. And after being contacted by KHN, Melissa Suggs, a spokesperson with Carlsbad Medical Center, said the facility is revising their lab charges.
“Pricing for these services will be lower in the future,” Suggs said in a statement.
Bill of the Month is a crowdsourced investigation by KHN and NPR that dissects and explains medical bills. Do you have an interesting medical bill you want to share with us? Tell us about it!
The recent rollout of two newly authorized COVID-19 vaccines is a bright ray of hope at the pandemic’s darkest hour.
We now have a path that can lead us to happier times — even as we watch and suffer from the horrible onslaught of new infections, hospitalizations and deaths that mark the end of this regrettable year.
Health care workers and nursing home residents have already begun to get shots in the first phase of the rollout. Vaccinations should start to be available to the general public sometime in the first few months of next year.
The two vaccines — one developed by Pfizer and BioNTech, the other by Moderna — use the same novel genetic approach. Their development in under a year, shattering all records, is a marvel of science. It’s also a cause for concern for millions of Americans who fear the uncertainty of an unknown technology.
The clinical trial data for the Pfizer and Moderna vaccines show that when both shots of the dual-injection immunization are taken, three weeks to a month apart, they are about 95% effective — at least at preventing severe COVID illness.
However, “a vaccine that remains in the vial is 0% effective no matter what the data show,” says Dr. Walter Orenstein, a professor of infectious diseases at the Emory University School of Medicine in Atlanta and associate director of the Emory Vaccine Center.
Hence, the imperative of persuading millions of people, across racial, cultural, religious, political and generational lines, to get immunized when a vaccine becomes available to them. A survey published this month showed 45% of respondents are taking a wait-and-see approach to vaccination.
Because the vaccines were developed under duress as the coronavirus exacted its deadly toll, the premium was on speed — “warp speed.” So although the number of people in the trials is as large as or larger than in previous vaccine trials, some key questions won’t be answered until millions more are vaccinated.
For example, we don’t know to what extent the vaccines will keep us from transmitting or contracting the virus — though the protection from potentially fatal illness they are likely to confer is in itself something of a miracle.
We don’t know whether irreversible side effects might emerge, or who is at higher risk from them. And we don’t know whether we’ll need to get vaccinated every year, every three years, or never again.
These unknowns add to the challenges faced by the federal government, local health authorities, medical professionals and private sector entities as they seek to persuade people across the broadest possible swath of the population to get a vaccine.
Skepticism resides in many quarters, including among African Americans, many of whom have a long-standing mistrust of the medical world; the vocal “anti-vaxxers”; and people of all stripes with perfectly understandable doubts. Not to mention communities with language barriers and immigrants without documents — more than 2 million strong in California — who may fear coming forward.
Here are answers to some questions you might be asking yourself about the new vaccines:
Q: How can I be sure they’re safe?
There’s no ironclad guarantee. But the federal Food and Drug Administration, in authorizing the Moderna and Pfizer vaccines, determined that their benefits outweighed their risks.
The side effects observed in trial participants were common to other vaccines: pain at the injection site, fatigue, headache, muscle pain and chills. “Those are minor side effects, and the benefit is not dying from this disease,” says Dr. George Rutherford, a professor of epidemiology at the University of California-San Francisco.
Saturday, the Centers for Disease Control and Prevention reported six cases of anaphylactic allergic reaction in the first 272,000 people who got the Pfizer vaccine outside the clinical trials. This has led the CDC to recommend that people receiving the vaccine be observed for up to 30 minutes afterward.
It’s possible other unexpected adverse effects could pop up down the road. “The chances are low, but they are not zero,” says Orenstein. There’s not enough data yet to know if the vaccines pose an elevated risk to pregnant or lactating women, for example, or to immunocompromised people, such as those with HIV. And we know very little about the effects in children, who were not in the initial trials and for whom the vaccines are not authorized.
Q: Why should my family and I take it?
First of all, because you will protect yourselves from the possibility of severe illness or even death. Also, by getting vaccinated you will be doing your part to achieve a vaccination rate high enough to end the pandemic. Nobody knows exactly what percentage of the population needs to get inoculated for that to happen, but infectious disease experts put the number somewhere between 60% and 70% — perhaps even a little higher. Think of it as a civic duty to get your shots.
Q: So, when can I get mine?
It depends on your health status, age and work. In the first phase, already underway, health care workers and nursing home residents are getting vaccinated. The 40 million Moderna and Pfizer doses expected to be available by year’s end should immunize most of them.
Next in line are people 75 and older and essential workers in various public-facing jobs. They will be followed by people ages 65-74 and those under 65 with certain medical conditions that put them at high risk. Enough vaccine could be available for the rest of the population by late spring, but summer or even fall is more likely. Already, some distribution bottlenecks have developed.
On the bright side, two other vaccines — one from Johnson & Johnson, the other from AstraZeneca and Oxford University — could win FDA authorization early next year, significantly increasing the supply.
Q: Once I’m vaccinated, can I finally stop wearing a mask and physical distancing?
No. Especially not early on, before a lot of people have been vaccinated. One reason for that is self-protection. The Moderna and Pfizer vaccines are 95% effective, but that means you still have a 5% chance of falling ill if you are exposed to someone who hasn’t been vaccinated — or who has been but is still transmitting the virus.
Another reason is to protect others, since you could be the one shedding virus despite the vaccination.
Q: I’ve already had COVID-19, so I don’t need the vaccine, right?
We don’t know for sure how long exposure to the virus protects you from reinfection. Protection probably lasts at least a few months, but public health experts say it’s a good idea to get vaccinated when your turn comes up — especially if it’s been many months since you tested positive.
There’s been some talk among health officials of pushing those who’ve been infected in the last 90 days or so toward the back of the line, to ensure adequate supply for those who might be at higher risk.
Q: How long before our lives get back to normal?
“If everything goes well, next Thanksgiving might be near normal, and we might be getting close to that by the summer,” says Dr. William Schaffner, a professor of infectious diseases at the Vanderbilt University School of Medicine in Nashville, Tennessee. ”But there would have to be substantial acceptance of the vaccine and data showing the virus moving in a downward direction.”
COVID-19 was the dominant — but not the only — health policy story of 2020. In this special year-in-review episode of KHN’s “What the Health?” podcast, panelists look back at some of the biggest non-coronavirus stories. Those included Supreme Court cases on the Affordable Care Act, Medicaid work requirements and abortion, as well as a year-end surprise ending to the “surprise bill” saga.
This week’s panelists are Julie Rovner of KHN, Joanne Kenen of Politico, Anna Edney of Bloomberg News and Sarah Karlin-Smith of Pink Sheet.
Among the takeaways from this week’s podcast:
The coronavirus pandemic strengthened the hand of ACA supporters, even as the Trump administration sought to get the Supreme Court to overturn the federal health law. Many people felt it was an inopportune time to get rid of that safety valve while so many Americans were losing their jobs — and their health insurance — due to the economic chaos from the virus.
Preliminary enrollment numbers released by federal officials last week suggest that more people were taking advantage of the option to buy coverage for 2021 through the ACA marketplaces than for 2020, even in the absence of enrollment encouragement from the federal government.
The ACA’s Medicaid expansion had a bit of a roller-coaster ride this year. Voters in two more states — Oklahoma and Missouri — approved the expansion in ballot measures, but the Trump administration continued its support of state plans that require many adults to prove they are working in order to continue their coverage. The Supreme Court has agreed to hear a challenge to that policy. Although lower courts have ruled that the Medicaid law does not allow such restrictions, it’s not clear how the new conservative majority on the court will view this issue.
Concerns are beginning to grow in Washington about the near-term prospect of the Medicare trust fund going insolvent. That can likely be fixed only with a remedy adopted by Congress, and that may not happen unless lawmakers feel a crisis is very near.
The Trump administration has sought to bring down drug out-of-pocket expenses for Medicare beneficiaries. Among those initiatives is a demonstration project to lower the cost of insulin. About a third of Medicare beneficiaries will be enrolled in plans that offer reduced prices in 2021. But the effort could have a hidden consequence: higher insurance premiums.
Many members of Congress began this session two years ago with grand promises of working to lower drug prices — but they never reached an agreement on how to do it.
President Donald Trump, however, was strongly motivated by the issue and late this year issued an order to set many Medicare drug prices based on what is paid in other industrialized nations. Drugmakers detest the idea and have vowed to fight it in court. Although some Democrats endorse the concept, it seems unlikely that President-elect Joe Biden would want to spend much capital in a legal battle for a plan that hasn’t been carefully vetted.
The gigantic spending and COVID relief bill that Congress finally approved Monday includes a provision to protect consumers from surprise medical bills when they are unknowingly treated by doctors or hospitals outside their insurance network. The law sets up a mediation process to resolve the charges, but the process favors the doctors. Insurers are likely to pass along any extra costs to consumers through higher premiums.
Workers at Garfield Medical Center in suburban Los Angeles were on edge as the pandemic ramped up in March and April. Staffers in a 30-patient unit were rationing a single tub of sanitizing wipes all day. A May memo from the CEO said N95 masks could be cleaned up to 20 times before replacement.
Patients showed up COVID-negative but some still developed symptoms a few days later. Contact tracing took the form of texts and whispers about exposures.
By summer, frustration gave way to fear. At least 60 staff members at the 210-bed community hospital caught COVID-19, according to records obtained by KHN and interviews with eight staff members and others familiar with hospital operations.
The first to die was Dawei Liang, 60, a quiet radiology technician who never said no when a colleague needed help. A cardiology technician became infected and changed his final wishes — agreeing to intubation — hoping for more years to dote on his grandchildren.
Few felt safe.
Ten months into the pandemic, it has become far clearer why tens of thousands of health care workers have been infected by the virus and why so many have died: dire PPE shortages. Limited COVID tests. Sparse tracking of viral spread. Layers of flawed policies handed down by health care executives and politicians, and lax enforcement by government regulators.
All of those breakdowns, across cities and states, have contributed to the deaths of more than 2,900 health care workers, a nine-month investigation by over 70 reporters at KHN and The Guardian has found. This number is far higher than that reported by the U.S. government, which does not have a comprehensive national count of health care workers who’ve died of COVID-19.
The fatalities have skewed young, with the majority of victims under age 60 in the cases for which there is age data. People of color have been disproportionately affected, accounting for about 65% of deaths in cases in which there is race and ethnicity data. After conducting interviews with relatives and friends of around 300 victims, KHN and The Guardian learned that one-third of the fatalities involved concerns over inadequate personal protective equipment.
Many of the deaths occurred in New York and New Jersey, and significant numbers also died in Southern and Western states as the pandemic wore on.
Workers at well-funded academic medical centers — hubs of policymaking clout and prestigious research — were largely spared. Those who died tended to work in less prestigious community hospitals like Garfield, nursing homes and other health centers in roles in which access to critical information was low and patient contact was high.
Garfield Medical Center and its parent company, AHMC Healthcare, did not respond to multiple calls or emails regarding workers’ concerns and circumstances leading to the worker deaths.
So as 2020 draws to a close, we ask: Did so many of the nation’s health care workers have to die?
New York’s Warning for the Nation
The seeds of the crisis can be found in New York and the surrounding cities and suburbs. It was the region where the profound risks facing medical staff became clear. And it was here where the most died.
As the pandemic began its U.S. surge, city paramedics were out in force, their sirens cutting through eerily empty streets as they rushed patients to hospitals. Carlos Lizcano, a blunt Queens native who had been with the New York City Fire Department (FDNY) for two decades, was one of them.
He was answering four to five cardiac arrest calls every shift. Normally he would have fielded that many in a month. He remembered being stretched so thin he had to enlist a dying man’s son to help with CPR. On another call, he did chest compressions on a 33-year-old woman as her two small children stood in the doorway of a small apartment.
“I just have this memory of those kids looking at us like, ‘What’s going on?’”
After the young woman died, Lizcano went outside and punched the ambulance in frustration and grief.
The personal risks paramedics faced were also grave.
More than 40% of emergency medical service workers in the FDNY went on leave for confirmed or suspected coronavirus during the first three months of the pandemic, according to a study by the department’s chief medical officer and others.
In fact, health care workers were three times more likely than the general public to get COVID-19, other researchers found. And the risks were not equally spread among medical professions. Initially, CDC guidelines were written to afford the highest protection to workers in a hospital’s COVID-19 unit.
Yet months later, it was clear that the doctors initially thought to be at most risk — anesthesiologists and those working in the intensive care unit — were among the least likely to die. This could be due to better personal protective equipment or patients being less infectious by the time they reach the ICU.
Instead, scientists discovered that “front door” health workers like paramedics and those in acute-care “receiving” roles — such as in the emergency room — were twice as likely as other health care workers to be hospitalized with COVID-19.
For FDNY’s first responders, part of the problem was having to ration and reuse masks. Workers were blind to an invisible threat that would be recognized months later: The virus spread rapidly from pre-symptomatic people and among those with no symptoms at all.
In mid-March, Lizcano was one of thousands of FDNY first responders infected with COVID-19.
At least four of them died, city records show. They were among the 679 health care workers who have died in New York and New Jersey to date, most at the height of the terrible first wave of the virus.
“Initially, we didn’t think it was this bad,” Lizcano said, recalling the confusion and chaos of the early pandemic. “This city wasn’t prepared.”
Neither was the rest of the country.
An Elusive Enemy
The virus continued to spread like a ghost through the nation and proved deadly to workers who were among the first to encounter sick patients in their hospital or nursing home. One government agency had a unique vantage point into the problem but did little to use its power to cite employers — or speak out about the hazards.
Health employers had a mandate to report worker deaths and hospitalizations to the Occupational Safety and Health Administration.
When they did so, the report went to an agency headed by Eugene Scalia, son of conservative Supreme Court Justice Antonin Scalia who died in 2016. The younger Scalia had spent part of his career as a corporate lawyer fighting the very agency he was charged with leading.
Its inspectors have documented instances in which some of the most vulnerable workers — those with low information and high patient contact — faced incredible hazards, but OSHA’s staff did little to hold employers to account.
Beaumont, Texas, a town near the Louisiana border, was largely untouched by the pandemic in early April.
That’s when a 56-year-old physical therapy assistant at Christus Health’s St. Elizabeth Hospital named Danny Marks called in sick with a fever and body aches, federal OSHA records show.
He told a human resources employee that he’d been in the room of a patient who was receiving a breathing treatment — the type known as the most hazardous to health workers. The CDC advises that N95 respirators be used by all in the room for the so-called aerosol-generating procedures. (A facility spokesperson said the patient was not known or suspected to have COVID at the time Marks entered the room.)
Marks went home to self-isolate. By April 17, he was dead.
The patient whose room Marks entered later tested positive for COVID-19. And an OSHA investigation into Marks’ death found there was no sign on the door to warn him that a potentially infected patient was inside, nor was there a cart outside the room where he could grab protective gear.
The facility did not have a universal masking policy in effect when Marks went in the room, and it was more than likely that he was not wearing any respiratory protection, according to a copy of the report obtained through a public records request. Twenty-one more employees contracted COVID by the time he died.
“He was a beloved gentleman and friend and he is missed very much,” Katy Kiser, Christus’ public relations director, told KHN.
OSHA did not issue a citation to the facility, instead recommending safety changes.
The agency logged nearly 8,700 complaints from health care workers in 2020. Yet Harvard researchers found that some of those desperate pleas for help, often decrying shortages of PPE, did little to forestall harm. In fact, they concluded that surges in those complaints preceded increases in deaths among working-age adults 16 days later.
One report author, Peg Seminario, blasted OSHA for failing to use its power to get employers’ attention about the danger facing health workers. She said issuing big fines in high-profile cases can have a broad impact — except OSHA has not done so.
“There’s no accountability for failing to protect workers from exposure to this deadly virus,” said Seminario, a former union health and safety official.
A database of deaths compiled by KHN and The Guardian includes a significant minority under 30, leaving shattered dreams and devastated families. (Photo Credit: The Obra family)
Home health aides flattened the curve by keeping the most vulnerable patients — seniors, the disabled, the infirm — out of hospitals. But they’ve done it mostly at poverty wages and without overtime pay, hazard pay, sick leave or health insurance. (Photo Credit: Tamarya Burnett)
By Danielle Renwick, The Guardian | August 27, 2020
Immigrant health workers help keep the U.S. health system afloat — and they’re dying of COVID-19 at high rates. (Photo Credit: Pablo Monsalve/VIEWpress via Getty Images)
An investigation by KHN and The Guardian shows that 329 health care workers age 65 or older have reportedly died of COVID-19. (Photo Credits: Tom Miles, David Brown, Bethany MacDonald)
Desperate for Safety Gear
There was little outward sign this summer that Garfield Medical Center was struggling to contain COVID-19. While Medicare has forced nursing homes to report staff infections and deaths, no such requirement applies to hospitals.
Yet as the focus of the pandemic moved from the East Coast in the spring to Southern and Western states, health care worker deaths climbed. And behind the scenes at Garfield, workers were dealing with a lack of equipment meant to keep them safe.
Complaints to state worker-safety officials filed in March and April said Garfield Medical Center workers were asked to reuse the same N95 respirator for a week. Another complaint said workers ran out of medical gowns and were directed to use less-protective gowns typically provided to patients.
Staffers were shaken by the death of Dawei Liang. And only after his death and a rash of infections did Garfield provide N95 masks to more workers and put up plastic tarps to block a COVID unit from an adjacent ward. Yet this may have been too late.
The coronavirus can easily spread to every corner of a hospital. Researchers in South Africa traced a single ER patient to 119 cases in a hospital — 80 among staff members. Those included 62 nurses from neurology, surgical and general medical units that typically would not have housed COVID patients.
By late July, Garfield cardiac and respiratory technician Thong Nguyen, 73, learned he was COVID-positive days after he collapsed at work. Nguyen loved his job and was typically not one to complain, said his youngest daughter, Dinh Kozuki. A 34-year veteran at the hospital, he was known for conducting medical tests in multiple languages. His colleagues teased him, saying he was never going to retire.
Kozuki said her father spoke up in March about the rationing of protective gear, but his concerns were not allayed.
Dinh Kozuki’s father, Thong Nguyen, died of COVID-related complications after nearly 35 years of service at Garfield Medical Center in Los Angeles. Nguyen’s supervisor told him he’d have to reuse personal protective equipment. “He definitely should not have passed [away],” Kozuki said.(Heidi de Marco / KHN)
The PPE problems at Garfield were a symptom of a broader problem. As the virus spread around the nation, chronic shortages of protective gear left many workers in community-based settings fatally exposed. Nearly 1 in 3 family members or friends of around 300 health care workers interviewed by KHN or The Guardian expressed concerns about a fallen workers’ PPE.
Health care workers’ labor unions asked for the more-protective N95 respirators when the pandemic began. But Centers for Disease Control and Prevention guidelines said the unfitted surgical masks worn by workers who feed, bathe and lift COVID patients were adequate amid supply shortages.
Mary Turner, an ICU nurse and president of the Minnesota Nurses Association, said she protested alongside nurses all summer demanding better protective gear, which she said was often kept from workers because of supply-chain shortages and the lack of political will to address them.
“It shouldn’t have to be that way,” Turner said. “We shouldn’t have to beg on the streets for protection during a pandemic.”
At Garfield, it was even hard to get tested. Critical care technician Tony Ramirez said he started feeling ill on July 12. He had an idea of how he might have been exposed: He’d cleaned up urine and feces of a patient suspected of having COVID-19 and worked alongside two staffers who also turned out to be COVID-positive. At the time, he’d been wearing a surgical mask and was worried it didn’t protect him.
Yet he was denied a free test at the hospital, and went on his own time to Dodger Stadium to get one. His positive result came back a few days later.
As Ramirez rested at home, he texted Alex Palomo, 44, a Garfield medical secretary who was also at home with COVID-19, to see how he was doing. Palomo was the kind of man who came to many family parties but would often slip away unseen. A cousin finally asked him about it: Palomo said he just hated to say goodbye.
Palomo would wear only a surgical mask when he would go into the rooms of patients with flashing call lights, chat with them and maybe bring them a refill of water, Ramirez said.
Paramedics work behind an ambulance at the Garfield Medical Center in Monterey Park, California, on March 19. (Frederic J. Brown / AFP via Getty Images)
Ramirez said Palomo had no access to patient charts, so he would not have known which patients had COVID-19: “In essence, he was helping blindly.”
Palomo never answered the text. He died of COVID-19 on Aug. 14.
And Thong Nguyen had fared no better. His daughter, a hospital pharmacist in Fresno, had pressed him to go on a ventilator after seeing other patients survive with the treatment. It might mean he could retire and watch his grandkids grow up. But it made no difference.
“He definitely should not have passed [away],” Kozuki said.
Nursing Homes Devastated
During the summer, as nursing homes recovered from their spring surge, Heather Pagano got a new assignment. The Doctors Without Borders adviser on humanitarianism had been working in cholera clinics in Nigeria. In May, she arrived in southeastern Michigan to train nursing home staffers on optimal infection-control techniques.
Federal officials required worker death reports from nursing homes, which by December tallied more than 1,100 fatalities. Researchers in Minnesota found particular hazards for these health workers, concluding they were the ones most at risk of getting COVID-19.
Pagano learned that staffers were repurposing trash bin liners and going to the local Sherwin-Williams store for painting coveralls to backfill shortages of medical gowns. The least-trained clinical workers — nursing assistants — were doing the most hazardous jobs, turning and cleaning patients, and brushing their teeth.
She said nursing home leaders were shuffling reams of federal, state and local guidelines yet had little understanding of how to stop the virus from spreading.
“No one sent trainers to show people what to do, practically speaking,” she said.
As the pandemic wore on, nursing homes reported staff shortages getting worse by the week: Few wanted to put their lives on the line for $13 an hour, the wage for nursing assistants in many parts of the U.S.
The organization GetusPPE, formed by doctors to address shortages, saw almost all requests for help were coming from nursing homes, doctors’ offices and other non-hospital facilities. Only 12% of the requests could be fulfilled, its October report said.
And a pandemic-weary and science-wary public has fueled the virus’s spread. In fact, whether or not a nursing home was properly staffed played only a small role in determining its susceptibility to a lethal outbreak, University of Chicago public health professor Tamara Konetzka found. The crucial factor was whether there was widespread viral transmission in the surrounding community.
“In the end, the story has pretty much stayed the same,” Konetzka said. “Nursing homes in virus hot spots are at high risk and there’s very little they can do to keep the virus out.”
The Vaccine Arrives
From March through November, 40 complaints were filed about the Garfield Medical Center with the California Department of Public Health, nearly three times the statewide average for the time. State officials substantiated 11 complaints and said they are part of an ongoing inspection.
For Thanksgiving, AHMC Healthcare Chairman Jonathan Wu sent hospital staffers a letter thanking “frontline healthcare workers who continue to serve, selflessly exposing themselves to the virus so that others may cope, recover and survive.”
The letter made no mention of the workers who had died. “A lot of people were upset by that,” said critical care technician Melissa Ennis. “I was upset.”
By December, all workers were required to wear an N95 respirator in every corner of the hospital, she said. Ennis said she felt unnerved taking it off. She took breaks to eat and drink in her car.
Garfield said on its website that it is screening patients for the virus and will “implement infection prevention and control practices to protect our patients, visitors, and staff.”
On Dec. 9, Ennis received notice that the vaccine was on its way to Garfield. Nationwide, the vaccine brought health workers relief from months of tension. Nurses and doctors posted photos of themselves weeping and holding their small children.
At the same time, it proved too late for some. A new surge of deaths drove the toll among health workers to more than 2,900.
And before Ennis could get the shot, she learned she would have to wait at least a few more days, until she could get a COVID test.
She found out she’d been exposed to the virus by a colleague.
Shoshana Dubnow and Anna Sirianni contributed to this report. Video by Hannah Norman Web production by Lydia Zuraw
This story is part of “Lost on the Frontline,” an ongoing project from The Guardian and Kaiser Health News that aims to document the lives of health care workers in the U.S. who die from COVID-19, and to investigate why so many are victims of the disease. If you have a colleague or loved one we should include, please share their story.

 16:36
16:36
 Annapoorna
Annapoorna